


Originally printed in the American Journal of Clinical Medicine, July 1921, pp. 437-443.
The “editorial comment” paragraph below is by the editor of the journal above.
EDITORIAL COMMENT — To be able to do without one’s eyeglasses, to read and write, to see at a distance, to recognize one’s friends and enemies (debtors and creditors) across the street — to eliminate the, not inconsiderable, item of expense for broken lenses, new frames; not to speak of repeated visits to the ophthalmologist — ’tis a consummation devoutly to be wished. Doctor Bates asserts that it can be done. His article, following below, and his book, reviewed on page 491 of this issue of Clinical Medicine, show how. Surely, Doctor Bares’ experiments and observations have been continued sufficiently long to merit consideration.
Table of Contents
Intro
At the very beginning of my practice as an ophthalmologist, I noticed that patients with myopia often recovered their vision spontaneously. This was not a new observation. Every ophthalmologist had noted such cases, but it was customary to explain them away. If a case of myopia recovered, a mistake in diagnosis had been made. Donders, had declared that myopia was incurable and, if the facts contradicted Donders, so much the worse for the facts. Donders himself set the example for this course by explaining away the cases of cured myopia reported by van Hasner. Von Hasner was a man of eminence for whose accuracy Donders expresses great respect; but, when it came to the cure of myopia, this respect did not prevent him from questioning the correctness of his observations. Some of van Hasner’s cases. he states, were reported in such a way that they lost all value as proofs and, in one case, he suggests that spasm of the accommodation had previously existed or that myosis had followed.
I had sufficient confidence in my ability to diagnose errors of refraction, however, to believe that, when a patient to whom I had given glasses for myopia came back to complain that they did not fit him, and was found to have normal vision, he really had been cured of myopia. f could not take refuge in the theory of mistaken diagnosis.

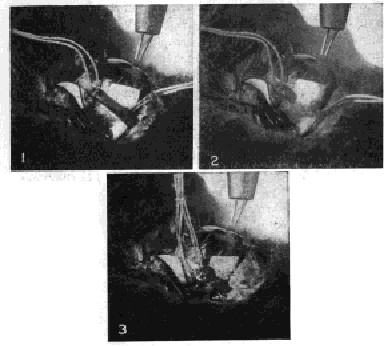
1 – The inferior oblique muscle has been exposed and two sutures are attached to it. Electrical stimulation of the eyeball produces accommodation as demonstrated by simultaneous retinoscopy.
2 – The muscle has been cut. Electrical stimulation produces no accommodation.
3 – The muscle has been sewed together. Electrical stimulation produces normal accommodation.
What was true of myopia, was true of other errors of refraction. They persisted in disappearing or in changing their degree, after having been carefully diagnosed under atropine, and I was unable to explain these facts on the basis of any of the accepted theories. This was particularly true in the case.of corneal astigmatism; for, the current explanations could not be made to apply at all to changes in this condition. Still less was I able to explain the well-known fact that some people can produce temporary corneal astigmatism at will. If the shape of the cornea could be changed at will from normal to abnormal and back again to normal, evidently something was wrong with the theory that astigmatism was due to a permanent deviation from the normal in the shape of the eyeball.
Errors of Refraction Not Permanent
Instead of being explained away and ignored, it seemed to me that such facts ought to be investigated. On seeking fight upon them, I examined an incredible number of eyes. In the course of time, I learned by the aid of simultaneous retinoscopy that not only astigmatism but any error of refraction could be produced at will. I also discovered that myopia is not, as we have so long believed, associated with the use of the eyes at the near-point but with a strain to see distant objects, while strain at the near-point produces hypermetropia. I became able, too, to cure the lower degrees of refractive error and to improve the higher ones. Out of deference to the teachings of the authorities, however, I continued for a long time to differentiate between functional myopia, which I was able to cure, and organic myopia, which I believed to be incurable. At late as 1912, in an address before the New York County Medical Society, I made this distinction.
Soon afterward, however, I learned, again by the aid of simultaneous retinoscopy, using the instrument at a distance of six feet or further, that no error of refraction was ever permanent, for, under certain conditions, the highest degrees of these errors would temporarily disappear. By this time, I had come to the conclusion that the whole problem of accommodation and errors of refraction needed to be reinvestigated. For the purpose of obtaining more light upon it, I undertook, about seven years ago, a series of experiments upon the eye muscles of fish, rabbits, cats and dogs, full details of which may be found in’the New York Medical journal for May 8, 1915. In these experiments, I was able, by manipulation of the external eye muscles, to produce and prevent accommodation and errors of refraction at will.
Experimental Observations
When two oblique muscles were present and active, accommodation was always produced, as measured by the objective test of retinoscopy, by electrical stimulation of the eyeball or of the nerves of accommodation near their origin in the brain. It was also produced by any manipulation of the oblique muscles whereby their pull was increased, as, by a tucking operation or by an advancement of the point at which they are attached to the sclerotic. But, after one or both of the obliques had been across or after they had been paralyzed by the injection of atropine deep into the orbit, accommodation could never be produced by electrical stimulation. After the effects of the atropine had passed away, however, or a divided muscle had been sewed together, accommodation followed electrical stimulation as before. Again, when one oblique muscle was congenitally absent or rudimentary, as was sometimes found to be the case, accommodation could not be produced by electrical stimulation. Yet, when the rudimentary muscle was strengthened by advancement or the absent one was replaced by a suture which sup. plied the necessary countertraction, accommodation could always be produced by electrical stimulation. (Fig. 1.)
In some of these experiments, the upper wall of the orbit was removed; and, whenever accommodation had been produced, either by electrical stimulation or by an operation upon the muscles, the eyeball was found to have elongated, indicating that the eye adjusts itself for near vision just as the camera does, namely, by lengthening its axis. This elongation was demonstrated by measurement and is shown in the accompanying photograph. (Fig. 2.)
Additional evidence of the relation of the oblique muscles to accommodation was found in the response of the fourth cranial nerve to electrical stimulation. In most textbooks on physiology, it is stated that accommodation is controlled by the third cranial nerve which supplies all the muscles of the eyeball except the superior oblique and the external rectus; but, in my experiments, the fourth nerve, which supplies only the superior oblique, was found to be just as much a nerve of accommodation as the third.

Fig. 2 – Demonstration Upon the Eyeball of a Rabbit That the Obliques Lengthen the Visual Axis in Myopia. Page 46, Fig. 18.
R, rest. The eyeball is of normal length and emmetropic – that is, perfectly adjusted for distant vision. My, myopia. The pull of the oblique muscles has been strengthened by advancement and the retinoscope shows that myopia has been produced. It can easily be noted that the eyeball is longer. It was impossible to avoid some movement of the head between the taking of the two pictures as a result of the manipulation of the strings, but the rule shows that the focus of the camera was not appreciably changed by such movements.
The Lens Not Concerned
The removal of the lens had no effect upon accommodation. In one experiment, the lens was removed from the right eye of a rabbit, the refraction of each eye having been first tested by retinoscopy and found to be normal. The wound was then allowed to heal. Thereafter, for a period of two years electrical stimulation always produced accommodation the lensless eye precisely as in the eye which had a lens. The animal was exhibited at a meeting of the Ophthalmoiogical Section of the American Medical Association, in Atlantic City, and was examined by a number of ophthalmologists present, all of whom testified that electrical stimulation of the lensless eyeball produced accommodation precisely as in the normal eye.
The recti muscles were found to be concerned in the production of hypermetropia. After one or both of the oblique muscles had been cut and while two or more of the recti were present and active, electrical stimulation of eyeball or of the nerves of accommodation always producd hypermetropia while by the manipulation of one of the recti, usually the inferior or superior, so as to strengthen its pull, the same result could be produced. The paralysing of the recti by atropine, or the cutting of one or more of them, prevented the production of hypermetropic refraction by electrical stimulation; but, after the effects of the atropine had passed away or after a divided muscle had been sewed together, hypermetropia was produced as usual by electric stimulation.
It should be emphasized that, in order to paralyse either, the recti muscles or the obliques, it was found necessary to inject the atropine far back behind the eyeball with a hypodermic needle. This drug is supposed to paralyze the accommodation when dropped into the eyes of human beings or of animals, but it was found in all my experiments that, when used in this way, it had very little effect upon the power of the eye to change its focus.
Astigmatism was usually produced in combination with myopia or hypermetropi refraction. It was also produced by various manipulations of both the oblique and recti muscles. Mixed astigmatism was always produced by traction on the insertion of the superior and inferior rectus in a direction parallel to the plane of the iris, as long as both obliques were present and active; but, if either or both of the obliques had been cut, the myopic part of the astigmatism disappeared, and, if the superior or inferior rectus had been cut, the hypermetropic part disappeared. Advancement of the two obliques, with advancement of the superior and inferior rectus, always produced mixed astigmatism.
Conclusions from Experimental Results
All of these experiments were repeated many times and always with the same result. Scientific men who witnessed them said that they were without sources of error. I was unable, therefore, to escape the conclusion that: The lens has nothing whatever to do with accommodation; the change of focus necessary for near vision is dependent upon the action of the oblique muscles; and, errors of refraction are produced by the abnormal action of the external muscles.
In Opposition to Helmholtz
As this conclusion was diametrically opposed to that reached by Helmholtz on his studies of images reflected from the front of the lens, I determined to repeat the experiments of the great German and find out, if possible, why his results were so different from my own. I devoted four years to this work and was able to demonstrate that Helmholtz had erred through a defective technic, the image obtained by his method being so variable and uncertain that it lends itself to the support of almost any theory.
Helmholtz used for his experiments: first, a small, bright light so laced that it was reflected from the cornea and the two-surfaces of the lens; then, two lights — or one doubled by reflection from a mirror — so placed behind a diaphragm having two rectangular openings that the rays shone through the openings upon the cornea and lens. Of the image obtained with the single unscreened light, he said that it was “usually so blurred that the form of the flame could not be definitely distinguished.” When the two lights with the diaphragm were used, the images were clearer, rod it seemed to him that, when the eye accommodated, they grew smaller and approach each other. This change, he said, could be seen “easily and distinctly.”
I was unable, however, by either of these methods, to obtain images that were sufficiently clear or distinct to be measured or photographed. With a naked candle as a source of light, a clear and distinct image could be obtained on the cornea; on the back of the lens it was quite clear; but, oil the front of the lens it was very imperfect. Not only was it blurred, just as Helmholtz had said, but, without any ascertainable cause, it varied greatly in size and intensity. At times, no reflection could be obtained at all, regardless of the angle of the light to the eye of the subject or of the eye-of the observer to that of the subject. With a diaphragm, I got a clearer and more constant image, but it still was not sufficiently reliable to be measured. Men who had been teaching and demonstrating the theory of Helmholtz repeated his experiments for my benefit, but the images which they obtained upon the front of the lens did not seem to me any better than my own. After studying these appearances daily for more than a year I was unable to make any reliable observation regarding them. With a thirty-watt lamp, a fifty-watt lamp, a 250-watt lamp and a 1000-watt lamp, there was no improvement. The light of the sun, reflected from the front of the lens, produced an image just as cloudy and uncertain as the reflections from other sources of illumination, and just as variable in shape, intensity and size. To sum it all up, I was convinced that the anterior surface of the lens was a very poor reflector of light and that no reliable images could be obtained by the means described.
The Difference Explained
I now began to work at an aquarium on the eyes of fish. After many failures, I became able, with the aid of a strong light (1000-watts), a diaphragm with a small opening, and a condenser, to obtain, after some difficulty, a clear and distinct image from the cornea of these animals. This image was sufficiently distinct to be measured, a satisfactory photograph being obtained after many months. Then, work was resumed on the eyes of human beings. The strong light combined with the diaphragm and condenser proved to be a decided improvement over the method of Helmholtz and, by means of this technique, an image was at last obtained on the front of the lens which was sufficiently clear and distinct to be photographed. This was the first time, so far as published records show, that an image of any kind was ever photographed from the front of the lens. Professional photographers, whom I consulted with a view to securing their assistance, assured me that the thing could not be done, and declined to attempt it. I was therefore obliged to learn photography myself, of which I had previously known nothing, and I then found that, as far as the image obtained by the method of Helmholtz is concerned, the professionals were right.
The experiments were continued until I obtained satisfactory pictures before and after accommodation and during the production of myopia and hypermetropia, not only of images on the front of the lens, but of reflections from the iris, cornea, the front of the sclera and the side of the sclera. I also became able to obtain reflections on any surface at will without reflections from the other parts. This was not done, however, until many difficulties lead been overcome, among which were the complicating reflections illustrated. (Fig. 3.)

This picture illustrates one of the difficulties that had to be overcome in photographing images reflected from various parts of the eyeball. Unless the light was adjusted at precisely the right angle the filament was multiplied by reflection from the sides of the globe. Usually the image was doubled, sometimes it was tripled, as shown in the picture, and sometimes it was quadrupled. Often days of labor were required to eliminate these reflections, and for reasons that were not definitely determined the same adjustment did not always give the same results Sometimes all would go well for days, and then, without any apparent reason, the multiple images would return.
The images photographed from the front of the lens did not show any change in size or form during accommodation. The image on the back of the lens also remained unchanged as observed through the telescope of the ophthalmometer; however, as there is no dispute about its behavior during accommodation, it was not photographed. Images photographed from the iris before and during accommodation were also the same in size and form, as was to be expected from the character of the lens images. If the lens changed during accommodation, the iris, which rests upon it, would change also. (Fig. 4.)

R, rest; A, accommodation. Under the magnifying glass no change can be observed in the size of the two images. The image at the right looks larger only because it is more distinct. To support the theory of Helmholtz it ought to be the smaller. The comet’s tail at the left of the two images is an accidental reflection from the cornea. The spot of light beneath is a reflection from the light used to illuminate the eye while the photographs were being taken. It took two years to get these pictures.
The images photographed from the cornea and from the front and side of the sclera showed, however, a series of four well-marked changes according to whether the vision was normal or accompanied by a strain. During accommodation, the images from the cornea were smaller than when the eye was at rest, indicating the elongation of the eyeball and a consequent increase in the convexity of the cornea. But, when an unsuccessful effort was made to see at the near-point, the images became larger, indicating that the cornea had become less convex, a condition which one would expect when the optic axis was shortened, as in hypermetropia.
When effort was made to see at a distance, the image was smaller than when the eye was at rest, again indicating elongation of the eyeball and inreased convexity of the cornea (Fig, 5.) The images photographed from the front of the sclera showed the same series of changes as the corneal images; but those obtained from the side of the sclera were found to have changed in exactly the opposite manner, being larger where the former were smaller and vice versa, a difference which one would naturally expect from the fact that, when the front of the sclera becomes more convex the sides must become flatter. When an effort was made to see at a distance, the image reflected from the side of the sclera was larger than the image obtained when the eye was at rest, indicating that this part of the sclera had become less convex, or flatter, because of elongation of the eyeball. The image obtained during normal accommodation was also larger than when the eye was at rest, indicating again a flattening of the side of the sclera. The image obtained, however, when an effort made to see near was much smaller than any of the images, indicating that the sclera had become more convex at the side, a condition which one would expect when the eyeball was shortened, as in hypermetropia. (Fig. 6.)

R, rest; A, accommodation. During accommodation the front of the sclera becomes more convex, because the eyeball has elongated, just as a camera is elongated when it is focussed upon a near object. The spot of light on the cornea is an accidental reflection.

R, rest; A, accommodation. The image in A is the larger, indicating a flattening of the side of the sclera as the eyeball elongates. My, Myopia. The eye is straining to see at the distance and the image is larger, indicating that the eyeball has elongated, resulting in a flattening of the side of the sclera. Hy, Hypermetropia. The eye is straining to see at two inches. The image is the smallest of the series, indicating that the eyeball has become shorter than in any of the other pictures, and the side of the sclera more convex. The two lower pictures confirm the author’s previous observations that farsight is produced when the eye strains to see near objects and nearsight when it strains to see distant objects.
The most pronounced of the changes was noted in the images reflected from the from of the sclera. Those on the side of the sclera were less marked, and, owing to the difficulty of photographing a white image on a white background, could not always be readily seen in the photographs. They were always plainly apparent, however, to the observer and subject. The alterations in the size of the corneal image were so light that they were not always observable, except when the image was large, a fact which explains why the ophthalmometer, with its small image, has been thought to show that the cornea did not change during accommodation.
Practical Results
The results of these experiments, which were first reported in The New York Medical Journal for May 18, 1918, were not only in harmony with the results of my experiments upon the eye muscles, but they confirmed my earlier clinical observations as to the causes of myopia and hypermetropia, and convinced me that the science of ophthalmology is a far more hopeful one than we have heretofore believed. According to the accepted teaching, myopia, hypermetropia and astigmatism are due to permanent deviations from the normal in the shape of the eyeball, while presbyopia is attributed to the hardening of the lens and is considered as being one of the unavoidable ills of advancing years. The foregoing experiments, combined with my clinical experiences, taught me that all of these conditions are due to a functional derangement in the outside muscles of the eyeball and are, therefore, both preventable and curable. I have since then been able to cure or improve all such cases, no matter how high their degrees or how long their duration. If the treatment has been continued long enough, the patient has been cured.
The cause of the abnormal action of the muscles has been shown to be a strain, or effort, to see. This strain originates necessarily in the mind. Therefore, all methods of treatment have for their object the attainment of mental relaxation. This is accomplished in various ways.
The mere closing of the eyes for a few minutes is often sufficient to improve the sight noticeably and some people have been cured by alternately resting the eyes for a few minutes in this way and then looking at the Snellen test card for a few seconds. A still greater degree of rest can be obtained in most cases by covering the eyes with the palms of the hands so as to exclude all the light. If perfect relaxation is gained in this way, one sees a perfect black, so black that it is impossible to remember, imagine, or see, anything blacker. At the beginning, though, patients often see bright lights and colors, and usually see grey. The use of the memory and imagination is a great help in obtaining relaxation. It is impossible to remember or imagine anything perfectly unless the mind is entirely relaxed, and, when the patient becomes able to remember or imagine perfectly even such a simple thing as a small black spot or period, the eye muscles relax and the sight becomes normal. Another method of gaining relaxation is to imitate consciously the unconscious shifting of the normal eye and to realize the apparent movement or swing produced by this shifting. The normal eye never holds a point more than a fraction of a second. When, however, the vision is imperfect, it has invariably been found that the eye tries to hold its points of fixation for an appreciable length of times Iz other words, it stares. This produces a great strain which is relieved by conscious shifting. Temporary relaxation can usually be obtained very quickly by these methods, and permanent relaxation, which means a permanent cure, is a mere matter of continued practice.
The same treatment has been found effective in many other conditions heretofore regarded as almost if not quite incurable, such as squint, amblyopia, cataract, glaucoma, atrophy of the optic nerve and retinitis pigmentosa. It is useful in many nervous conditions, and is miraculously effective in relieving pain.
Citations
- The pages and figures refer to Doctor Bates’ book on the same subject, which is reviewed on page 491 of this issue – Editor.
get help on our Facebook Group!




In the early 20th century, Dr. Bates began noticing that the vision of some patients would vary and that some would see better after not having worn their glasses or by resting their eyes in certain ways. Through many years of clinical and experimental work, he learned what things are restful to the eyes and cause the vision to improve, and what things cause vision to worsen and even cause further complications with the eyes.